
Functionality and use of design
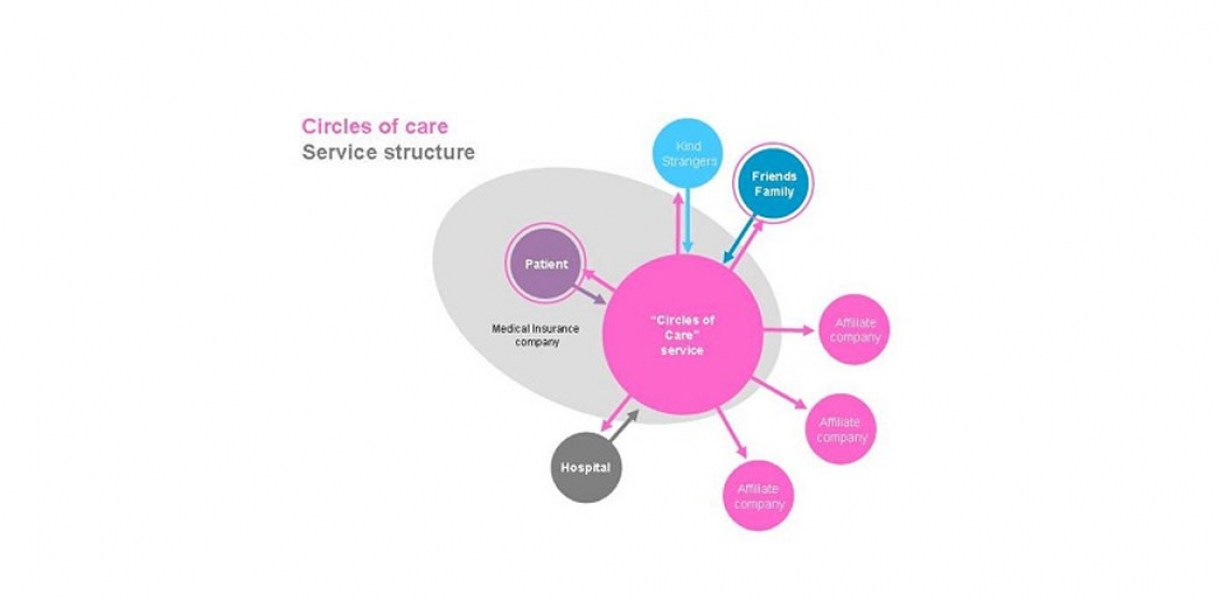
The service mediates the relationship between the hospital patient and their social circle. Using ICT, friends & family can provide comforts, participate in events remotely and maintain flows of communication with the patient. The service is personal, adaptive to local conditions and accessible through a variety of technologies.
How did this design improve life?
“Very cool idea, especially because of an ever-increasing global community was definitely going to use the service. It would be useful for me personally as my family is spread out all over the globe.“ Vincent, A test user, Cape Town
Our lives are increasingly becoming more flexible, connected and mobile. In contrast, hospitalization involves dependency, immobility and isolation. Everyday life is disrupted. Our aim was to maintain a continuum of a person’s social, family and work life while hospitalized. We were looking for ways to help patients retain a sense of normality in an extreme situation. We believe that communication with loved ones and small, timely comforts can make a big difference in the patient’s life and is the core of the service we have designed.
Our solutions cater for the following needs:
1. Keeping the continuum of social and family life while hospitalized. Close friends organize a TV night with the patient, which allows them to communicate in real-time over remote locations.
2. Catering to distant relationships and social obligations. A colleague orders a gift from the patient's wish list and has it delivered to the patient’s bedside.
3. Bridging distance/keeping group identity. Family and friends record a get-well song to be delivered to the patient in a hospital without the chorus members having to be in the same place at the same time.
4. Caring for strangers Anyone can choose comforts from wish lists that were made by lonely people, and send improve their hospital experience by giving them something they want.
The service should be scalable to local conditions and accessible through a variety of technologies. It should also offer a variety of long and short-term solutions to cater for varying lengths of hospitalization.
We believe the strength of our service is the framing of existing solutions (delivery of goods, scheduling and communication) around a clearly defined social network - the friends and family of the hospitalized patient. This framing makes the service operate on a personal level and allows needs to drive the commercial functions.
The potential benefit is not only for the users but also for possible stakeholders such as medical insurance companies who might sponsor the service. Having happier patients also mean reducing the costs of their hospitalization. It is a known fact that psychological factors affect patients’ physical condition and that patients with a positive attitude are likely to recover faster from their illness.
This service has been conceived and developed for the specific case of the hospital. The general concept and also some specific ideas could easily be applied to other situations/contexts such as elderly homes, student campus, and in many situations in which people live far away from their loved ones.
Drawbacks of life improvement
What if I am not part of the service?
In designing our service we tried to be as inclusive as possible. Circles of Care should not be perceived as an exclusive luxury service. It should allow the involved members to determine their own level of involvement and investment. For example, services and goods available to the patient should fall in a fixed price range. Also, people who are listed as part of your circle of care do not have to be members of the service to benefit from it.
What if I do not have a social circle to call on?
Our service assumes that the patient has an existing social network of friends and family to support him during the hospitalization. To cater to the lonely patient, our service also allows ‘kind strangers’ to provide comforts to patients they do not know.
What about my privacy?
Our service relies on making patient information available to his/her close friends and family. Making sensitive data available to the outside brings up privacy concerns. Our service tries to counter this by giving the patient complete control over who is being informed. Our service also makes use of service representatives located at the hospitals which form a ‘human interface’ between the patient and the outside. “Circles of Care” therefore takes the responsibility of a trusted third party.
How will our service effect hospital resources?
Our service positions itself as the trusted third party that is responsible for patient care. It, therefore, becomes responsible for the well-being of the patient while in the hospital. This takes some responsibility from hospital staff and becomes s support rather than a burden. Having service representatives on location at the hospital will ensure that services brought in from outside (catering, delivery etc.) can be dealt with in an efficient manner.
Research and need
This project was about examining design in the context of “people & health”, learning about social networks and service design. We looked at the way people act, communicate and connect in health-related situations. The social-cultural-local environment was an active design factor and we did not only look at designing for the individual, but designing for communities of people and the social networks that surround them.
Our research included the following methods: secondary research, brainstorming techniques, knowledge mapping, user observation, In-depth Interviews, cultural probes, Experience prototypes.
Circles of care: Self explorations with PosIt notes
Everyone is surrounded by people, objects and institutes that support them in times of need. We call them "circles of care". To learn more about their meaning in our lives we started by mapping the roles of the different circles of care according to various health conditions (chronic situation, light illness, emergency, hospitalization).
We came up with two main areas which we wanted to investigate further: patient empowerment and maintaining the continuum of the patient's life while hospitalized.
Interviews and photo elicitation
We conducted 8 in-depth open-ended interviews with people from different nationalities. We also used cameras as cultural probes that were given to the interviewees beforehand.
Our learnings were:
• “You have your right to have your little things… the hospital can’t cut your life completely. That’s awful”. Maria, 68, Italy.
• “I didn’t want people to visit me… I just wanted things to be different”. Silvia, 35, Italy.
• “I think it depends on where people are at, in the course of their illness. In the beginning, it was really tiring to even read a newspaper”. Linda, 56, US.
Experience Prototype
We created experience prototypes to test our service on the side of the patient as well as the friends and family.
Prototype 1
To test our service with the family and friends we created a Circles of Care service for our very own Interaction Design Institute Ivrea (IDII) community. We pretended as if Ruth and Bernd were hospitalized in Ivrea and emailed friends and family to offer their support through our service. Touch-points included emails, websites of Bernd and Ruth's personalized wish lists and a comment page which allowed the users to send us comments about our service.
Reaction: “Very cool idea, especially because of ever-increasing global community was definitely going to use the service. It would be useful for me personally as my family is spread out all over the globe”. Vincent, test user, Cape Town
Prototype 2
With our second prototype we wanted to test our service on a patient. For this we went to the local hospital and presented a patient called Carlo with our Circles of Care catalogue. He told us that he really would enjoy salami. We left the hospital and made our way to the nearest market. An hour later, with the approval of the hospital staff, we presented the patient with his salami.
Carlo's reaction: "This is amazing! They made my day! I have to call my wife!”
Our research helped us define the following guidelines for the service:
- Utilize existing social networks
- Make it a scalable service (it works in Ivrea, it works in Milan)
- Make it accessible through various technologies: fax, phone, mobile, internet
- Come up with a variety of long and short-term services
- Offer information about the patient's condition
- Don't make it feel like e-commerce
- Make it personal and socially sensitive
Designed by
Bernd Hitzeroth, Ruth Kikin-Gil & Steven Blyth (Italy), 2004